






Introduction
What is malaria?
Malaria has been recognized as a human disease for thousands of years and remains one of the most common diseases affecting humans worldwide. Malaria impact falls almost entirely on developing countries, with the heaviest toll in Africa. Over half the world’s population is thought to be exposed to the risk of contracting malaria. As well as its direct health cost, it carries a significant economic burden in countries where there is endemic disease:
- Malaria slows economic growth in Africa, fuelling the vicious cycle which perpetuates poverty .
- In Africa, it accounts for 40% of public health expenditure and 7% of the household income .
- Malaria deters investment, tourism and labour-intensive cash-crops.
During the 1960s and 1970s, there was optimism that malaria could be eradicated. The 1980s and 1990s saw serious setbacks, such as the development of resistance to commonly used drugs and insecticides as well as the breakdown of control programmes and local primary health services, often in the context of regional political and economic collapse. Child deaths due to malaria doubled in sub-Saharan Africa in the 1990s and malaria re-emerged in Central Asia, Eastern Europe and previously clear areas of Southeast Asia.
The Roll Back Malaria Partnership (RBMP) is a global partnership of countries committed to the eradication of malaria. To this end, the RBMP recently published Action and Investment to defeat Malaria 2016-2030 (AIM) – for a malaria-free world and this compliments the WHO Global Technical Strategy for Malaria 2016-2030
Economic Burden and Impact
Malaria not only exacts a direct toll on human health but also imposes a significant economic burden, predominantly felt in developing countries. The disease hampers economic growth in Africa, perpetuating a vicious cycle of poverty. Beyond its direct health costs, malaria impedes investment, tourism, and the cultivation of labor-intensive cash crops.
Historical Perspectives
While the optimism of the 1960s and 1970s hinted at the eradication of malaria, subsequent decades witnessed setbacks. The emergence of drug and insecticide resistance, coupled with the breakdown of control programs, led to a resurgence of malaria in regions previously hopeful for its elimination. Child mortality in sub-Saharan Africa doubled in the 1990s, and malaria re-emerged in areas considered malaria-free.
Global Initiatives: Roll Back Malaria Partnership
The Roll Back Malaria Partnership (RBMP), a global alliance, is dedicated to malaria eradication. Recently, the RBMP published “Action and Investment to defeat Malaria 2016-2030 (AIM),” aligning with the World Health Organization’s Global Technical Strategy for Malaria 2016-2030. These initiatives aim for a malaria-free world through strategic planning and coordinated efforts.

Economic Impact of Malaria
- Cycle of Poverty: Malaria contributes to the perpetuation of poverty in affected regions.
- Public Health Expenditure: In Africa, it accounts for 40% of public health expenditure.
- Household Income: Malaria affects 7% of household income in affected areas.
Historical Timeline of Malaria
- 2700 BC: Described by the Chinese in the Nei Ching (the Canon of Medicine).
- 340 AD: The use of the qing hoa plant (sweet wormwood) for fever was described.
- 1971: Identification of artemisinin, the active ingredient in modern antimalarial drugs.
- 19th Century: Malaria was endemic in the marshes of Southern and Eastern England.

Aetiology
Malaria is a parasitic disease caused by infection by species of the genus Plasmodium.
| Clinical features | UK cases 2014 |
|
| Plasmodium falciparum | Responsible for severe disease and malaria-related deaths. Incubation 7-14 days (up to one year if semi-immune); most travellers present within eight weeks. Classical tertian and subtertian periodicity (paroxysms at 48- and 36-hour intervals) are rare; daily (quotidian) or irregular are more common. |
1169 |
| Plasmodium vivax | Causes benign tertian malaria – fever every third day. Incubation period of 12-17 days. Relapse due to dormant parasites in the liver. |
225 |
| Plasmodium ovale | Relapsing course as with P. vivax. Incubation period of 15-18 days. |
130 |
| Plasmodium malariae | Causes benign quartan malaria – fever every fourth day – but this is frequently not observed, particularly in early infection. Long incubation period (18-40 days). Parasites can remain dormant in the blood. 5-10% present over a year after infection. With chronic infection, can cause nephrotic syndrome. |
41 |
A fifth species causing malaria in humans, Plasmodium knowlesi, has recently emerged. It is distributed across Southeast Asia and is often misdiagnosed by microscopy as P. malariae. However, it is potentially more serious, causing severe malaria with a rate of 6-9% and with a case fatality rate of 3%.
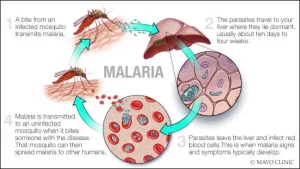
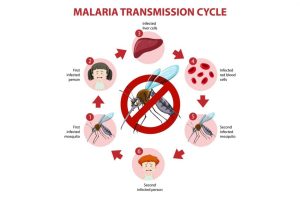
Humans acquire malaria after being bitten by an infected mosquito. The sporozoites in the saliva of the mosquito then travel via the bloodstream to the liver where they mature or, in certain species, may lie dormant (when they are known as hypnozoites). The mature organisms then rupture to release further organisms (merozoites) into the blood, where they invade red blood cells and undergo asexual reproduction. Feeding mosquitoes ingest these in a blood meal and in the mosquito gut they undergo sexual reproduction to produce thousands of infective sporozoites, and the cycle continues.
Understanding Malaria: Causes and Transmission
Epidemiology and Global Impact
Malaria predominantly occurs in tropical and subtropical regions, with approximately half of the world’s population at risk. In 2015, there were around 214 million cases and 438,000 deaths, with sub-Saharan Africa bearing the majority of the burden. Despite the high figures, global efforts have led to a 60% reduction in mortality rates since 2000.
Risk Factors and Groups at Risk
- The Poor: 60% of deaths from malaria occur in the poorest 20% of the population.
- Young Children and Infants: Particularly vulnerable to severe disease.
- Pregnant Women: Especially primigravidae.
- Elderly People: Face increased risk.
- Non-immune Individuals: Such as travelers and foreign workers.
Malaria Presentation and Symptoms
Recognizing malaria in patients is crucial for timely treatment. Symptoms, including fever, chills, headache, and gastrointestinal upset, may appear from days to months after infection. Prompt diagnosis is essential to prevent complications and fatalities.
Malaria Signs and Severe Disease
- Fever: A common early sign of malaria.
- Splenomegaly: Enlargement of the spleen.
- Hepatomegaly: Enlargement of the liver.
- Jaundice: Yellowing of the skin and eyes.
- Abdominal Tenderness: May be present in severe cases.

Signs of Severe Disease (Usually P. falciparum)
- Impaired Consciousness
- Shortness of Breath
- Bleeding
- Fits
- Hypovolaemia
- Hypoglycaemia
- Acute Kidney Injury
- Nephrotic Syndrome
- Acute Respiratory Distress Syndrome (During Treatment)
Malaria Differential Diagnosis
As the initial symptoms of malaria are nonspecific, several alternative diagnoses may be considered. However, in returning travelers, these should only be investigated after excluding the possibility of malaria due to the serious consequences of a delay in diagnosis. Other travel-related infections that may present with similar symptoms include typhoid, hepatitis, dengue, influenza, HIV, meningitis/encephalitis, and viral hemorrhagic fevers.
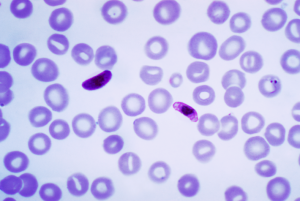
Diagnostic Investigations and Treatment
Accurate diagnosis through blood smears or rapid diagnostic tests is vital for effective case management. Treatment varies based on the severity and Plasmodium species involved. Severe cases often require hospital admission, and the choice of antimalarial drugs depends on the specific circumstances.
Non-falciparum Malaria
This is usually managed on an outpatient basis unless the patient has other comorbidities. G6PD activity should be measured in P. vivax or P. ovale infections, as the primaquine can cause hemolysis in those with G6PD deficiency.
Falciparum Malaria
Current UK guidelines suggest that all patients with falciparum malaria should be admitted to the hospital for the first 24 hours, as even semi-immune patients may worsen quickly. High-quality supportive management is important in patients with severe or complicated malaria.
Malaria Complications
Complications, almost always associated with P. falciparum infection, can be severe and life-threatening. Prompt treatment is crucial for a positive prognosis. Complications include impaired consciousness or seizures (cerebral malaria), renal impairment, acidosis, hypoglycemia, pulmonary edema or acute respiratory distress syndrome, anemia, splenic rupture, disseminated intravascular coagulopathy, shock secondary to complicating bacteremia/sepsis (algid malaria), hemoglobinuria (‘black water fever’), multiple organ failure, and death.
Malaria Prognosis
If no chemoprophylaxis has been taken, or if left untreated, or where treatment is delayed, malaria may be fatal. In the UK, there were 15 deaths reported in 2019. The mortality rate varies significantly with the species of Plasmodium causing the infection and the standard of care.
Malaria Prevention: A Multifaceted Approach
Preventing malaria involves a combination of chemoprophylaxis, insecticide-treated nets, and behavioral modifications. The World Health Organization recommends the use of the RTS,S malaria vaccine in endemic areas. Efforts to control and prevent malaria have a profound impact on reducing its global burden.
Prevention Strategies
- Chemoprophylaxis: Antimalarial drugs for travelers to endemic areas.
- Insecticide-Treated Nets: Provide effective protection against mosquito bites.
- Mosquito Avoidance: Use of repellents, long-sleeved clothing, and bed nets.
- Environmental Measures: Reduction of mosquito breeding sites.
- Malaria Vaccine: Implementation of the RTS,S malaria vaccine.

Historical Insights
Understanding the historical context of malaria reveals the intricate interplay between climate change, human resistance, and the development of treatments. From ancient Chinese descriptions to the discovery of artemisinin and synthetic drugs, the battle against malaria has deep roots in human history.
Conclusion
In conclusion, malaria stands as a persistent global health challenge with profound economic and human impacts, particularly in developing nations. Despite setbacks, ongoing initiatives like the Roll Back Malaria Partnership and global prevention efforts have significantly reduced mortality rates. The multifaceted nature of malaria demands a comprehensive approach, combining historical insights with modern interventions. Accurate diagnosis, timely treatment, and preventive measures, including the innovative RTS,S malaria vaccine, play pivotal roles. As we delve into the historical roots of this ancient malady, the hope remains for a future where malaria is eradicated, sparing millions from its grasp.



